Adenomas Of The Liver
Liver disease is serious and requires treatment and regular monitoring by a liver specialist.
A liver specialist is known as a hepatologist and you need to be referred by your family doctor or general practitioner. Over nearly 40 years of practicing medicine I have seen many patients develop severe liver disease, which sadly could have been prevented by early detection and early referral to a hepatologist. There needs to be more awareness of liver disease so that patients can be treated early so that we can prevent cirrhosis, liver failure and liver cancer. Make sure you have your liver function checked annually with a blood test.
I have presented my ideas on how to help those with liver diseases using nutritional medicine, which I have been using for many years with good success rates. However my recommendations do not replace the care of your own doctor and you should remain under the care of your own doctor whilst using nutritional therapies.
If you have any questions you may contact my naturopath, Christine, on 623 334 3232 or email us at [email protected]
Since the 1980s liver cell adenoma and liver cell adenomatosis (multiple adenomas) have emerged as new entities in medical practice due to the widespread use of oral contraceptives and high dose hormone replacement therapy.
The increased prevalence of patients with liver cell adenoma is due to the widespread use of estrogen-based oral contraceptives, as well as the increased use of imaging tests (such as ultrasound scans and CAT scans) of the abdomen for a variety of unrelated reasons. This means that many adenoma tumors are identified as incidental findings in patients with no liver symptoms. The clinical importance and natural history of these incidental adenoma tumors is not fully understood, and there is a need for optimal management strategies in such patients.
The causal relationship between oral contraceptives and other oral estrogens and liver cell adenoma is proportional to the dose and duration of the hormone medication. The incidence is highest in women over 30 years of age after using oral contraceptives for more than 2 years. It is estimated that the risk of growing an adenoma increases by a factor of 5 after 5 years, and by 25 after 9 years of oral contraceptive usage.
Adenomas of the liver
Liver cell adenoma is a common and benign (non-cancerous) tumor of the liver. A liver adenoma is an encapsulated liver tumor (has a capsule around it) and it does not contain bile ducts.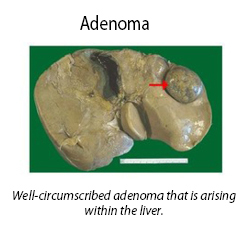 Causes of liver adenomas
Causes of liver adenomas
Since the 1980s liver cell adenoma and liver cell adenomatosis (multiple adenomas) have emerged as new entities in medical practice due to the widespread use of oral contraceptives and high dose hormone replacement therapy.
The increased prevalence of patients with liver cell adenoma is due to the widespread use of estrogen-based oral contraceptives, as well as the increased use of imaging tests (such as ultrasound scans and CAT scans) of the abdomen for a variety of unrelated reasons. This means that many adenoma tumors are identified as incidental findings in patients with no liver symptoms. The clinical importance and natural history of these incidental adenoma tumors is not fully understood, and there is a need for optimal management strategies in such patients.
The causal relationship between oral contraceptives and other oral estrogens and liver cell adenoma is proportional to the dose and duration of the hormone medication. The incidence is highest in women over 30 years of age after using oral contraceptives for more than 2 years. It is estimated that the risk of growing an adenoma increases by a factor of 5 after 5 years, and by 25 after 9 years of oral contraceptive usage.
Outcome of liver adenomas
Liver adenoma has a low possibility of bleeding into the liver. Transformation into liver cancer is rare; however this risk goes up if the adenoma has a diameter of over 5 centimetres. Pregnancy often stimulates rapid growth in liver adenomas with risk of potentially fatal spontaneous rupture and such patients should be referred to a top liver specialist.Diagnosis of liver adenoma
The best imaging technique is an MRI scan of the liver. If the adenoma is very large or looks suspicious for liver cancer, it can be biopsied for definite diagnosis.Treatment of liver adenoma
If the patient is on oral contraceptives or estrogen containing hormone replacement therapy it is vital to cease using them. This often results in the adenoma shrinking and oral contraceptive-induced liver cell adenomas are reversible if oral contraceptives are discontinued within a certain time period. With prolonged oral contraceptive usage, pre-cancerous changes (dysplastic foci) may develop within the adenoma that may progress to liver cancer. The causative role of oral estrogen containing contraceptives in producing liver cell adenoma is beyond doubt, and many studies have shown regression and even complete disappearance of adenomas after cessation of the oral contraceptive pill. Because adenoma has a risk of bleeding and malignant transformation, surgical excision is usually done for solitary liver adenomas.Liver cell adenomatosis
Liver cell adenoma caused by estrogen ingestion is usually solitary (one tumor only), but some people may develop several adenomas spread throughout the liver. This latter condition is known as liver cell adenomatosis and does not have the strong association with estrogen or anabolic steroid use. If the tumors are causing severe symptoms and are accessible to surgery, they should be surgically removed. Other treatments such as embolization (blocking the blood supply) to bleeding tumors and radiofrequency destruction may be useful in some patients.Follow up
Regular and long term medical supervision is vital because even complete disappearance of the adenoma does not prevent the later development of liver cancer, which has been observed five years after cessation of oral contraceptive usage and regression of the adenoma. There are no reports of new adenoma formation or development of liver cancer after surgical removal of solitary liver cell adenoma. In liver cell adenomatosis where there is extensive distribution of the lesions, management decisions are more problematic, as targeted adenoma excision is not an easy treatment. If there are many large tumor nodules ranging from 1 to 4 inches (2–10 cm) in diameter, then enlargement and deformation of the liver may occur. This is called a “massive type” and may be rapidly progressive and presents a real treatment challenge. The ‘multifocal type’ contains many adenomas up to 2 inches (4-5 cms) in diameter but the liver shape is not deformed or enlarged. These patients are unlikely to have many symptoms and appear to have a less aggressive clinical course. Patients should be entered into a follow up program that includes yearly CAT scans or MRI scans, and frequent serum alpha-fetoprotein (AFP) measurement in a blood test. AFP is a protein that is a marker for liver cancer and rising levels must be taken seriously. These tests are done to detect progression of disease (increased lesion size) and/or transformation into liver cancer. All female patients should be advised to stop hormone medication (e.g. oral contraceptives and hormone replacement therapy), and also ensure that they prevent further pregnancies. Those who have the massive form of liver cell adenomatosis may have multiple large lesions within a single lobe of the liver, and are best managed by partial removal of the liver. Patients with multifocal liver cell adenomatosis should be monitored with regular liver imaging. Progression of disease with larger adenomas, concern of malignant transformation, and increasing symptoms are indications for resection in multifocal liver cell adenomatosis. Resection is the preferable option unless technically impossible. Liver transplantation should be considered only as a last resort. Indications where liver transplantation is considered may include rise in serum alpha-fetoprotein, concern about transformation to cancer on scans, and patients with marked enlargement of the liver and repeated bleeding of the adenomas.Nutritional help for adenomas
In patients with liver adenomas, either solitary or multiple, it is important to have a healthy diet and to avoid eating sugar and refined carbohydrates. If you are overweight, a low carbohydrate diet that is free of all grains and refined sugar is important and may shrink tumors. This is because a low carbohydrate diet lowers insulin levels and insulin is a growth promoting hormone that can promote the growth of tumors. It is vital to support healthy liver function to try and shrink the adenomas; I recommend the following –- Selenomune Take one capsule daily with food. Selenium has been studied in large clinical trials and has a proven effect in reducing liver cancer. Selenomune is the leading selenium supplement available and contains the correct dose.
- Vitamin D3 Especially if you are low in blood levels of vitamin D.
- Super Vitamin K Take 2 capsules daily with food.
- N-Acetyl-Cysteine (NAC) Take 1 capsule twice daily.
Know someone who might benefit from this article? Share it!



18 Comments
Search
Shop Our Products by
Health Interest
-

Hormone & Thyroid Health
-

Liver & Gallbladder Health
-

Digestive Health
-

Bone & Joint Health
-

Women's Health
-

Immune Health
-

Healthy Aging
-

General Health
Most Recent Articles
Need Help?
1-888-75-LIVER
Monday to Friday, 9:00 am to 5:00 pm MST
100%
Satisfaction Guaranteed
If it’s faulty or wrongly described, we’ll replace it.
It sounds like you've been through a lot.
I hope you find the above article helpful.
Please check out Dr Cabot's video on liver cysts here:https://www.youtube.com/watch?v=jcJ_BLDM_ls
Please let us know how you get on.
Kind regards,
Jessah Shaw
Nutritionist
Oral contraceptive pill I used for 11 years. I stopped taking them a decade ago. My BMI is 22, I do not drink alcohol and excercise a lot, however in according to pictures I have a fatty liver. I have taken multiple iron infusions over the years due to anemia. Diabetes runs in the family. I have often pain under the rib cage, it feels like preassure.
After the tests I received the diagoses with a mentioning that a follow up would be good. How often does one need a follow up? Do I need a blood test for the liver markers too?
My family GP not to worry about the lesions. I have nothing serious as there was no malignacy detected. Should I demand to see a hepatologist?
Many thanks for your advise!
Please take our recommended supplements in the above article to shrink the adenomas: Selenomune, NAC, Vitamin K2 and Vitamin D.
It's also very important to follow a low-carb diet such as the one in Dr Cabot's book 'Fatty Liver: You Can Reverse It'.
It would be a good idea to get the adenomas monitored every 3 to 6 months. Up to you if you want to see a hepatologist. We recommend discussing with your healthcare practitioner.
Kind regards,
Jessah Shaw
Nutritionist
Liver specialist asked me stop with hormone therapy straight away, but still said I could use the progesterone part (utrogestan) and changed from ginet (combi pill) yo cerazette (progesterone pill) transition went ok, but now I’m experiencing terrible pain in hand and feet which makes me not being able to function at all, work is hard and sleeping because of pain is terrible. The exercise I need to do to loose a bit of wait to get BMI down is very much a struggle due to joint pains.
Anything g you suggest for this also I stopped all vitamin supplements and wet no carbs, no alcohol, almost no sugars, really clean foot and changed breakfast and dinner around. Any supplements you suggest I could take that would help assist my liver? And anything for the terrible pain in hands and feet so I can fu citron normally again? Thanks a million!
What is your email address?
Are you from the U.S?
Dr Cabot can email you directly.
Kind regards,
Jessah Shaw
Nutritionist
a liver adenoma needs to be monitored with 6 monthly ultrasound scans of the liver
it can be caused by the oral contraceptive pill.
if you also have a fatty liver change your diet - see my videos on fatty liver to see best way to eat for your liver or read my LIVER CLEANSING DIET book
To shrink the adenoma, I recommend LIVATONE PLUS 4 capsules daily
also vitamin D 5,000 IU Daily with food
Best wishes
Dr Sandra Cabot
A copper IUD creates a higher copper environment constantly while it is present, and does not increase the level at ovulation or after menstruation.
Ovulation is an inflammatory process and is often a sign of generalized inflammation.
Copper IUDs are often associated with heavier more painful periods.
Another benefit of the IUD is that adenomas are often associated with the use of the contraceptive pill, so your liver may heal with the change you have made.
Kind regards
Victoria
Naturopath for Dr Sandra Cabot MD
Adenomas are often stimulated by high estrogen levels which is often present with the use of OCP preparations or a high xenoestrogen load.
Adenomas are usually benign and resection is most often unnecessary and be assured that a biopsy will determine if the adenoma is suspicious.
Be aware that insulin stimulates the growth of tumors throughout the body, so please have your daughter begin a liver friendly anti-inflammatory diet like Dr Cabot’s 15 Day Cleanse and Maintenance Program.
Supplementation is also needed and Dr Cabot prescribes Selenommune, Vitamin D, Super Vitamin K, and NAC.
Kind regards
Victoria
Naturopath for Dr Sandra Cabot MD
But, my concern is the pain I feel and original reason I went to the gastro Dr isn't resolved: I continue to have this 1) nuisance pain underneath my rt breast and rib cage. There's also 2) pain and sometimes a lump can be felt between my ribs (lower last three rt side). But puzzling thing: we've been looking at this for almost 4 yrs and no resolution, but the adenomas has showed up ( oh and in 2017 randomly found out about a hemongonia ( sp?) on liver). So I am still at a loss in this regard. They say the adenomas
and hemp aren't connected. And they say neither should causing the pain I feel.... i can feel pain sometimes when I bend a certain
way, other times it just hurts. Sometimes it feels like a cooling affect inside, other times when I bath, I get a strange sensation. I don’t just know, I sometimes feel like I should try to reach out to those doctors who address "strange" medical cases. It def. feels like a Rollercoaster ride and I have no answers, but I do have this "new" information.
Open for any thoughts.
Adenomas are benign, as are hemangiomas, but they occupy space that the liver should be using for other detoxification tasks and yours may have increased in size to be able to do these tasks. An enlarged liver tends to produce pain under the right ribs.
To help resolve the cysts, ensure you are taking the smallest dose of contraceptive or HRT required as these are indicated as possible causes.
A liver friendly diet will help to reduce the size of your liver and as cysts shrink and liver returns to normal size we expect the pain to also resolve.
Livatone Plus is a beneficial supplement to add to those prescribed in the article.
Kind regards
Victoria
Jason’s story www. FiberWater.com/history.phpg
Thanks for sharing yours and Jasons story.
All the best :)
Louise
Good luck.
Kind regards,
Jessah Shaw
Nutritionist for Liverdoctor.com